Address Disparities
Eliminating health disparities benefits everyone!
Health equity exists when all people have the opportunity to access their full health potential. Health disparities develop when economic, social, or environmental conditions prevent a person from achieving their full health potential.
Whether or not someone uses tobacco is not just an individual choice. The factors that drive these disparities, are known and there are evidence-based strategies to solve them.1 Tobacco-related health disparities are a social injustice, in addition to a health and economic burden.
State and local efforts to extend programs and services to eliminate tobacco-related disparities will reduce the overall rate of commercial tobacco use in Washington state, improve quality of life and longevity, and contribute to health equity efforts.
Image Source: this Reality-Equality-Equity-Justice image is widely used and has been attributed to @restoringracialjustice. We thank its developer.
Our Focus
Washington Breathes recognizes that all communities are affected differently by commercial tobacco use across racial, ethnic, and socioeconomic groups. We support universal wellness strategies and tailored interventions to address health disparities and promote health equity in all communities.
| Learn more about our Shared Terminology on terms like equity, disparities, and inequities |
Surgeon General's Report on Tobacco-Related Disparities
The U.S. Surgeon General published a report in November 2024 on "Eliminating Tobacco-Related Disease and Death: Addressing Disparities," which explains the factors that drive tobacco-related health disparities and recommends strategies to end them.
Disparities in Commercial Tobacco Impacts
Progress has been made in reducing commercial tobacco use through regulations, education, and prevention strategies. However, as overall smoking rates decline, not all populations are equally protected or supported. For decades, tobacco-related disparities have persisted by race and ethnicity, levels of income and education, mental health conditions, sexual orientation and gender identity, and geography. Disparities in use and nicotine dependence result from a combination of factors1, including:
- targeting of specific communities by the commercial tobacco industry through disproportionate product marketing, sponsorships for cultural events, celebrity endorsements, and other tactics2;
- disparities in distribution of tobacco and vapor product retail locations, and
- contributing traumas, stressors and factors from social and economic injustices and other adverse experiences in these communities.
Policies and programs have contributed to these problems by not always providing culturally appropriate services or recognizing that specific communities need targeted strategies. Disparities in access to resources and services from many factors, including:
- differences in protection provided to different communities from laws and policies,
- differences in availability of resources, programs, and effective interventions for different communities, and
- inadequate recognition of community needs due to limitations in data collection and research design that overlook or undercount the impacts on specific subpopulations.
For example, the sale of menthol cigarettes fuels health disparities and inequities. More specifically, the rate of death and disease from menthol tobacco use in African American and Black communities has been devastating. In Washington State, use of menthol tobacco products is also higher in Native American and LGBTQ+ communities. In 2009, federal law prohibited the sale of all other flavored cigarettes, but menthol cigarettes remained on the market despite the disproportionate harm they cause to Black Americans.
2024 U.S. Surgeon General's Report on Addressing Disparities
A November 2024 report from the U.S. Surgeon General titled "Eliminating Tobacco-Related Disease and Death: Addressing Disparities"1 explains the factors that drive tobacco-related health disparities and recommends strategies to end them:
Key Report Findings -
Factors That Drive Disparities:
- Poverty, racism, discrimination, and other social determinants of health.
- The tobacco industry’s targeted marketing and promotion of commercial tobacco products—including menthol products—to certain population groups and poor neighborhoods.
- Gaps in protections by commercial tobacco prevention and control strategies, such as smoke and vape free air policies.
- Preemptive laws that prevent or block communities from protecting their members’ health through local regulations.
- Financial and other obstacles to accessing treatments proven to help people quit using tobacco.
Key Report Findings - Strategies to End Disparities:
- Remove social and structural obstacles to health equity, including poverty, racism, and discrimination.
- Make commercial tobacco products less appealing, addictive, affordable, and available.
- Decrease the tobacco industry’s influence on society.
- Apply evidence-based commercial tobacco prevention and control strategies everywhere, and for everyone.
- Increase access to treatments and resources to help people quit commercial tobacco use.
Government policies, like the following, can reduce disparities:
- Comprehensive smoke/vape free policies for all indoor areas of public places and workplaces, and multi-unit housing.
- Regulation of the amount of nicotine allowed in cigarettes, e-cigarettes, and other commercial tobacco products to make them less addictive or not addictive.
- Restrictions on the sale of flavored tobacco products, including menthol cigarettes and flavored cigars.
- Regulation of the location and number of stores that sell commercial tobacco products.
- Tobacco product price increases, through eliminating price discounts and increasing taxes.
- Support and promotion for quitlines and cessation services.
- High impact educational media campaigns that reach all communities.
Whether someone uses tobacco or not is the result of many different factors, as explained in this report. Learn more:
- Read the Full Report or a technical Executive Summary
- This Consumer Guide provides a useful summary of the data and the report's recommendations in a more graphical format. Spanish version of Consumer Guide
- CDC Presentation Slides (PDF)
- Tobacco Health Disparities Fact Sheet en español
Update: as of early February 2025, the CDC removed the webpage for the Surgeon General's report and resources to comply with Executive Orders. The full report and some resources are provided here from our Resources Library.
Data on Existing Disparities
In Washington State, communities of color, LGBTQ+, lower socioeconomic individuals, rural communities, veterans, and people with behavioral health concerns experience higher rates of tobacco use and related diseases. Expand each section to see data for each group on commercial tobacco use and health impacts:
Washington State Data
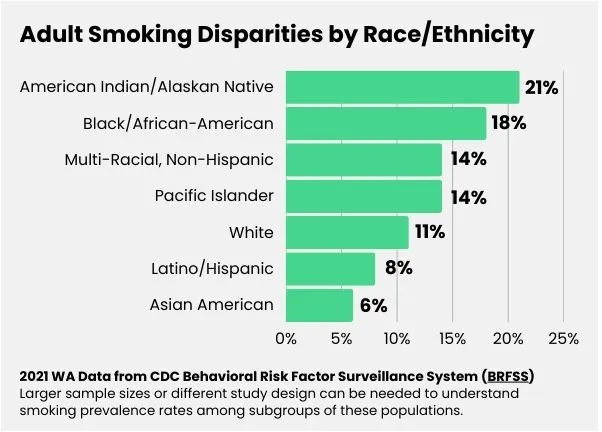
- Black/African-American Adult Smoking Rate: 18% compared to 11% overall WA smoking rate (2021 BRFSS).
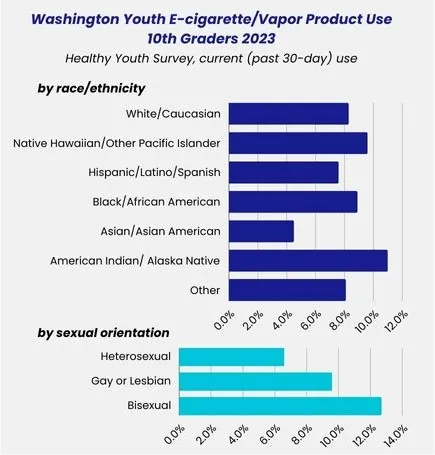
- Black/African-American Youth Vaping Rate - 10th grade: 8.9% compared to 7.7% overall WA youth rate (2023 WA Healthy Youth Survey)
- 56.5% of Black/African Americans who smoke in Washington use menthol cigarettes compared to 19.6% of white people. (Campaign for Tobacco-Free Kids, 2021 fact sheet, and 2021/2022 Behavioral Risk Factor Surveillance System Survey)
National Data
- Tobacco-related illness is the leading cause of preventable death for African-Americans. Over 95% of African-American Youth in the U.S. who smoke use menthol cigarettes (They Think They Know You)
- 85% of Black smokers use menthol cigarettes and 50% of teens age 12-17 use menthol cigarettes. (2018 National Survey on Drug Use and Health, cited in Delnevo et al. "Banning Menthol Cigarettes: A Social Justice Issue Long Overdue")
- If menthol cigarettes were banned nationally, research shows 44.5% of African Americans who smoke menthol would try to quit. (Truth Initiative 2020 fact sheet)
- Lung cancer death rates in Black males are 15% higher than those of white males. Prohibiting menthol tobacco products could close that gap in about 5 years. (Institute for Health Metrics and Evaluation, Council on Foreign Relations 2023)
Key Organizations
- Center for Multicultural Health: leading WA organization on commercial tobacco issues that effect the Black/African-American community
- African American Tobacco Control Leadership Council (AATCLC) leading organization working at intersection of social justice and public health policy for the African American and African Immigrant communities.
- The Center for Black Health and Equity: leading public health group that facilitates programs and services to promote health equity for people of African descent.
Resources
- African American People and Commercial Tobacco: Health Disparities and Ways to Advance Health Equity CDC webpage with information, data, and resources
Washington State Data
- American Indian/Alaskan Native Adult Smoking Rate: 21% compared to 11% overall WA smoking rate (2021 BRFSS)
- American Indian/Alaskan Native Youth Vaping Rate - 10th grade: 11.0% compared to 7.7% overall WA 10th grade vaping rate (2023 WA Healthy Youth Survey)
- 43.1% of American Indian/Alaska Natives who smoke in Washington use menthol cigarettes compared to 19.6% of white people. (2021/2022 Behavioral Risk Factor Surveillance System Survey)
National Data
- More than 1 in 4 (27.1% ) American Indian/Alaska Native adults smokes cigarettes. This is much higher than the overall national smoking rate of 12.5%. (2020 data from 2022 MMWR report)
- Estimated that 56% of American Indian and Alaska Native (AI/AN) want to quit (2020 Smoking Cessation: Report of the Surgeon General)
- AI/AN people, compared to the other racial and ethnic groups, have a higher risk of death and disease caused by using commercial tobacco products like cigarettes, smokeless tobacco, and cigars. (multiple sources cited on this CDC webpage)
Key Organizations
- American Indian Health Commission for Washington State: leading WA organization on commercial tobacco issues that effect the American Indian/Alaska Native community
- National Native Network: Keep It Sacred national network focused on reducing commercial tobacco-related illnesses and disparities; excellent source of information on traditional tobacco use by some American Indians and Alaskan Natives
Resources
- American Indian and Alaska Native People and Commercial Tobacco: Health Disparities and Ways to Advance Health Equity CDC webpage with information, data, and resources
- Unfair and Unjust Practices and Conditions Harm American Indian and Alaska Native People and Drive Health Disparities CDC webpage with information about historical and current policies and practices
Washington State Data
- Asian American Adult Smoking Rate: 6% compared to 11% overall WA smoking rate (2021 BRFSS)
- Pacific Islander Adult Smoking Rate: 14% compared to 11% overall WA smoking rate (2021 BRFSS)
- Native Hawaiian/Pacific Islander (NH/PI) Youth Vaping Rate - 10th grade: 9.6% compared to 7.7% overall WA 10th grade vaping rate (2023 WA Healthy Youth Survey)
- 49.4% of Native Hawaiian/Other Pacific Islanders and 26.2% of Asian Americans who smoke in Washington use menthol cigarettes compared to 19.6% of white people. (2021/2022 Behavioral Risk Factor Surveillance System Survey)
Larger sample sizes or different study designs are needed to better understand smoking prevalence rates among subgroups of these Asian-American populations. Learn more in this review by the Truth Initiative To fully understand tobacco use among AANHPI, representation in research matters (May 2024).
National Data
- In 2019, 77% of NH/PI and 4 out of 5 Asian adult smokers reported using a menthol brand, and
In 2011, over half of Asian youth aged 12-17 who smoked reported using a menthol brand, and
Filipino and Native Hawaiian/Pacific Islander adults who smoke are more likely to use menthol cigarettes than other groups of Asian adults.
(research cited on CDC webpage Unfair and Unjust Practices and Conditions Harm Asian, Native Hawaiian, and Pacific Islander People and Drive Health Disparities) - NH/PI youth had the highest vaping rates and second highest smoking rates among all racial/ethnic groups.
In 2014-2017, 45% of Native Hawaiian/Pacific Islander middle and high school students reported ever using any tobacco product, compared to 16.3% of Asian middle and high school students. (2018 CDC MMWR report) - 70% of Asian adults who smoke cigarettes want to quit (CDC Quitting Smoking Among Adults — United States, 2000–2015)
- Differences in cigarette smoking are seen among diverse Asian population groups. For instance, during 2010–2013, 7.6% of Chinese American adults smoked cigarettes, compared to 20% of Korean American adults. (research cited on CDC webpage Asian, Native Hawaiian, and Pacific Islander People Experience a Health Burden From Commercial Tobacco)
Key Organizations
- Asian Pacific Islander Coalition Advocating Together for Healthy Communities (APICAT): leading WA organization on commercial tobacco issues that effect the Asian Pacific Islander community
- Appeal (Asian Pacific Partners for Empowerment, Advocacy, and Leadership): National network that supports and mobilizes community-led movements for health equity and commercial tobacco control/prevention.
Resources
- Asian, Native Hawaiian and Pacific Islander People and Commercial Tobacco: Health Disparities and Ways to Advance Health Equity CDC webpage with information, data, and resources
- Invisible in the data: Broad ‘Asian American’ category obscures health disparities Nov. 21, 2023 STAT article about data equity and health equity, with links to many useful research studies
- Truth Initiative To fully understand tobacco use among AANHPI, representation in research matters (May 2024)
Washington State Data
- Hispanic/Latine Adult Smoking Rate: 8% compared to 11% overall WA smoking rate (2021 BRFSS)
- Hispanic Youth Vaping Rate - 10th grade: 7% compared to 7.6% overall 7.7% WA 10th grade vaping rate (2023 WA Healthy Youth Survey)
- 28.9% of Hispanic individuals who smoke in Washington use menthol cigarettes compared to 19.6% of white people. (2021/2022 Behavioral Risk Factor Surveillance System Survey)
Larger sample sizes or different study design can be needed to understand smoking prevalence rates among subgroups of these populations.
National Data
- 7.4% of Hispanic middle and high school students currently used any commercial tobacco product. (2021 National Youth Tobacco Survey)
- An estimated 67% of Hispanic adults who smoke cigarettes indicate wanting to quit (CDC Quitting Smoking Among Adults — United States, 2000–2015)
- In 2015, Hispanic adults who smoked were less likely to receive advice to quit from a healthcare professional than non-Hispanic white adults who smoked. And less likely to use an evidence-based cessation treatment (counseling or medication) than non-Hispanic white adults. (research cited on CDC webpage Hispanic and Latino People Encounter Barriers to Quitting Successfully)
Key Organizations
- ESD 123 and El Centro de la Raza: leading WA organizations on commercial tobacco issues that affect the Hispanic and Latino communities.
- National Latino Tobacco Control Network CDC funded national center to engage and empower Latinos on commercial tobacco control
- Nuestras Voces (Our Voices) Network CDC supported collaborative working to reduce commercial tobacco use and tobacco-related cancers
Resources
- Hispanic and Latino People and Commercial Tobacco Use: Health Disparities and Ways to Advance Health Equity CDC webpage with information, data, and resources
Washington State Data
- Gay, Lesbian, Bisexual Youth Vaping Rate - 10th grade: 12.7% among bisexual youth and 9.6% among gay or lesbian youth, compared to 7.7% overall WA 10th grade vaping rate (2023 WA Healthy Youth Survey)
- Current E-Cigarette Use (2021 WA BRFSS data): 12.3% for LGB adults compared to 5.6% for heterosexual adults.
- Current Cigarette Use 2019-2021: 12.1% for LGB adults compared to 11.8% for heterosexual adults. (WA BRFSS data analyzed by the WA State Department of Health)
- Current Smokeless Tobacco Use 2019-2021: 1.1% for LGB adults compared to 3.1% for heterosexual adults (WA BRFSS data analyzed by the WA State Department of Health)
BRFSS survey data was combined for several years to obtain a sufficient sample size. Larger sample sizes or different study design can be needed to understand smoking prevalence rates among subgroups of these populations. Questions used to identify sexual orientation/gender identity (SO/GI) also vary between different surveys.
National Data
- 40% of LGB youth used commercial tobacco in the last year. (2020 CDC MMWR report)
- People who identify as lesbian, gay, bisexual or transgender (LGBT) who smoke are more likely to smoke menthol cigarettes than heterosexual people who smoke. (research cited on CDC Menthol Smoking and Related Health Disparities webpage)
- 35% of transgender people are current smokers. (2020 Tobacco Prevention & Cessation)
Key Organizations
- Seattle’s LGBTQ+ Center: leading WA organization on commercial tobacco issues that affect the LBGTQ+ community
- National LGBT Cancer Network
- Smoking is a Social Justice Issue & we are fighting for our lives online info hub on tobacco industry tactics, menthol products, and the LGBTQ+ community from National LGBT Cancer Network
Resources
- Tobacco Use in LBGT Communities 2021 Truth Initiative report
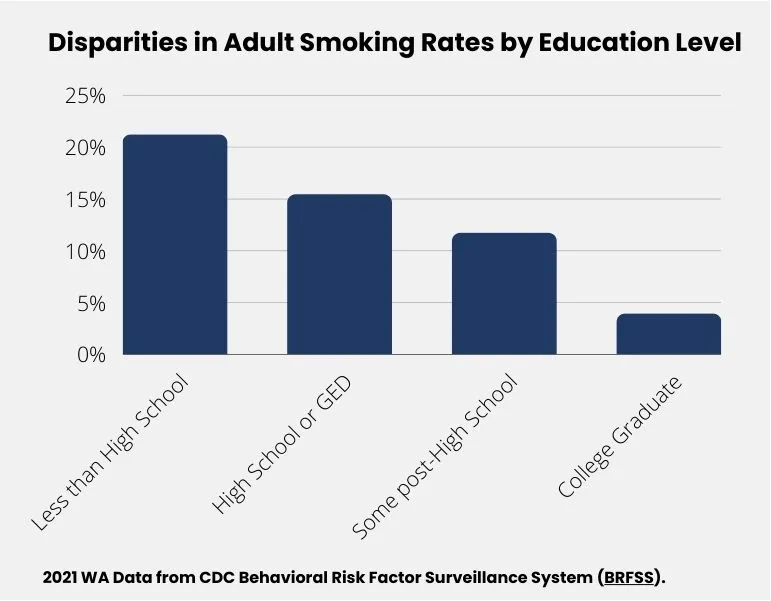
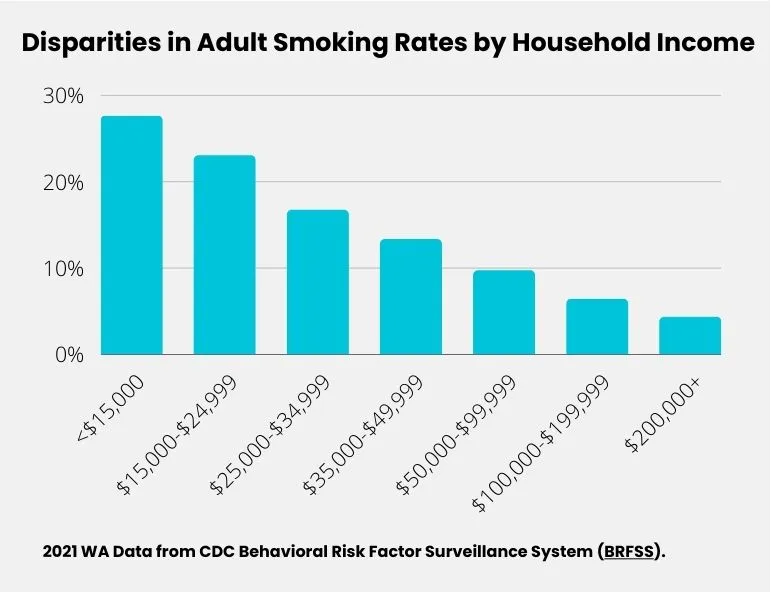
Use of commercial tobacco products is higher among people of lower income levels.
Washington State Data (2021 BRFSS)
- Adult Current Smoking Rate by Income:
- 0-$49,000 per year - 18%
- $50,000-$199,000 per year - 8%
- more than $200,000 per year - 4%
- Adult Current Smoking Rate by Employment Status:
- Employed for wages - 10%
- Unemployed for 1 or more years - 24%
- Unemployed for great than 1 year - 22%
- Unable to work - 32%
National Data
- 18.3% of adults living in low-income households smoke, compared to 12.3% of adults living in middle-income households, and 6.7% of adults living in high-income households. (2020 data from 2022 CDC MMWR report)
- People with lower income have higher incidence of commercial tobacco-related diseases than people with higher levels of income. (2022 Campaign for Tobacco-Free Kids Tobacco and Socioeconomic Status)
- Current commercial tobacco product use prevalence is higher among adults who were uninsured (27.3%), enrolled in Medicaid (28.6%), or had some other public insurance (21.3%) compared to adults with private insurance (16.4%) or Medicare only (12.5%). (2020 data from 2022 CDC MMWR report)
Resources
National Data
- Overall rates of vaping were higher among rural youth (8.4%) than for the non-rural youth (7.6%) in the 2023 Healthy Youth Survey. (Rural Washington Data from 2023 HYS, reviewed by Clark County Public Health)
- 19% of adults living in rural areas smoke compared to 11.4% among adults that live in urban areas. (CDC 2020 MMWR)
- Rural high school students are more likely to smoke cigarettes and use smokeless tobacco than high school students in urban areas. (NYTS data 2011-2016, Journal of Rural Health 2020)
Key Organizations:
- Statewide Rural Network leading network in Washington State building resilience and preventing youth substance misuse.
Resources
- Geographic Regions and Commercial Tobacco: Health Disparities and Ways to Advance Health Equity CDC webpage with information, data, and resources
- Rural Washington Data from 2023 HYS, reviewed by Clark County Public Health (May 2024)
Individuals with military or veteran status are known to have higher tobacco-use rates than the general population and more than a third of all active-duty smokers in the military start smoking after they enlist. (WA State Department of Veterans Affairs)
Military members and their families have unique challenges and barriers to successfully quit tobacco-use, such as frequent moves, deployment, and behavioral health issues linked to active military duty. These challenges and barriers often remain for individuals long after their transition from the military to civilian life.
Washington is home to more than 530,000 veterans, almost 12% of the state population. (WA State Department of Veterans Affairs)
In partnership with Washington State Department of Health and funded by a grant from The Centers for Disease Control (CDC), the Veterans Commercial Tobacco Cessation Program (DVA) exists to connect Washington’s veterans and military families to resources that help decrease tobacco dependence, increase cessation efforts, and provide support for staying stopped.
National Data
From 2010-2015 national data:
- 29.2% of veterans reported current use of any of the assessed commercial tobacco products.
- Cigarettes were the most commonly used commercial tobacco product (21.6%), followed by cigars (6.2%), smokeless tobacco (5.2%), roll-your-own tobacco (3.0%), and pipes (1.5%); 7.0% of veterans currently used two or more tobacco products.
- Within subgroups of veterans, current use of any of the assessed commercial tobacco products was higher among persons aged 18–25 years (56.8%), Hispanics (34.0%), persons with less than a high school diploma (37.9%), those with annual family income <$20,000 (44.3%), living in poverty (53.7%), reporting serious psychological distress (48.2%), and with no health insurance (60.1%).
- Commercial tobacco use was significantly higher among all veteran groups than their nonveteran counterparts, except males aged ≥50 years.
(CDC Tobacco Product Use Among Military Veterans — United States, 2010–2015)
Key Organizations
- Veterans Commercial Tobacco Cessation Program of the Washington State Department of Veterans Affairs
Resources
- Become a Smokefree Veteran CDC smokefree.gov
Washington State Data
- 28% of Washington adults with poor mental health smoke. (WA DOH)
- 58% of youth who smoke and 54% of youth who vape reported depression symptoms compared to 34% among youth who do not use commercial tobacco products. (2018 WA HYS data)
Analysis of 2018 Healthy Youth Survey data by ESD 112’s Prevention and Youth Services Department found correlation between commercial tobacco use and depression, marijuana use, alcohol use, and suicidal ideation. Smoking and vaping can indicate a need for social-emotional care and health supports.
Learn more about youth commercial tobacco use as a Red Flag for Supports.
National Data
- About 1 in 4 (25%) of U.S. adults have some form of mental illness or substance abuse disorder, and they account for 40% of all U.S. adult cigarette consumption. (CDC, 2020)
- People with mental health conditions who smoke cigarettes have two times the risk of premature death than people with behavioral health conditions who do not smoke. (Tam et al. Journal of Preventive Medicine. 2016)
Resources
- Understanding tobacco use and behavioral health. (WA Department of Health)
- Tobacco-Free Behavioral Health Initiative (WA Department of Health)
- “Red Flags for Support: Students Who Smoke or Vape” WA OSPI fact sheet
Improving Health Equity
Our coalition’s vision and mission focus intentionally on eliminating commercial tobacco-related inequities through policy, systems, and environmental changes. We work to improve health equity by:
- educating about tobacco industry targeting of communities, past and current commercial tobacco inequities, and resulting health disparities,
- examining and focusing on improving equity in the programs and policies we support,
- supporting the right of local communities to protect themselves from tobacco industry tactics, including local authority for stronger regulations to limit commercial tobacco sales and marketing,
- recognizing that people addicted to nicotine products are often coping with greater stressors and inequities than the general population and opposing programs or policies that blame or stigmatize them,
- supporting investments in culturally responsive strategies that are developed by each community to support their well-being, and
- identifying and trying to fill data gaps to understand impacts of commercial tobacco on specific communities and improving research infrastructure to be more representative and inclusive of all Washington communities.
Video: ‘Striving Towards Equity: A Scoping Review of E-Cigarettes, HTPs and Tobacco Related Disparities’ by The Institute for Global Tobacco Control at Johns Hopkins University.
Video Training: ‘Developing culturally relevant, multicultural, and inclusive communications with GMMB’ by The Rede Group for the YCCTPP

Additional Resources
- U.S. Department of Health and Human Services. "Eliminating Tobacco-Related Disease and Death: Addressing Disparities - A Report of the Surgeon General" https://www.cdc.gov/tobacco-surgeon-general-reports/about/2024-end-tobacco-disparities.html
- “Stopping Menthol, Saving Lives” report from multiple organizations. Feb. 2021. https://www.tobaccofreekids.org/what-we-do/industry-watch/menthol-report
- Teens and young adults in Washington believe that vaping is harmless (2021): Fact Sheet developed by APICAT and other key organizations working in diverse communities
- The Tobacco Atlas: Race, Ethnicity, and Equity (May 2022).
- “Associations Between Disparities in Tobacco Retailer Density and Disparities in Tobacco Use” Jan. 2022. Glasser et al. Prevention Medicine article through National Library of Medicine.
- Health Disparities Related to Commercial Tobacco and Advancing Health Equity (CDC).
- Unfair and Unjust Practices and Conditions Harm African American People and Drive Health Disparities (CDC).
- Truth Initiative: Across all 50 states, the same 5 disparities in cigarette smoking persist. (August 2024)
- Truth Initiative: To fully understand tobacco use among AANHPI, representation in research matters. (May 2024)